Elizabeth Jane Howard
Husbands, lovers and novels

Most obituaries of the author of The Cazalet Chronicles paid more attention to her beauty, marriages and affairs than to her writing. Married to Peter Scott (ornithologist and son of the polar explorer), James Douglas-Henry, and famously Kingsley Amis, she had affairs with Laurie Lee, Ken Tynan, Cecil Day-Lewis, Cyril Connolly, and Arthur Koestler. Bad boys all.
The Amis affair started off passionate and wonderful, but once they’d formalised the relationship, he expected her to wait on him hand and foot, took to heavy drinking, and probably not unrelated, became impotent. The best thing that came out of it was Martin Amis, who having been allowed to run wild by his mother Hilly and Kingsley, was allegedly put back on the straight and narrow by Jane. She deserves a better poem than this.
Young Elizabeth Jane
Had both beauty and brain,
The most high powered
Of the family Howard.
When an aged ornithologist
Held back the budding novelist,
She started up affairs with poets
And chronicled the Cazalets
But the poets’ ugly wives
Soon got out the sharpened knives,
So, after meeting Lucky Jim,
She jumped again, and married him
But although she mixed his drink
He kept her at the kitchen sink.
Soon, after Martin she was looking
While the boozer did the writing
Learning late that men are useless
She finally fulfilled her promise,
And the lesson of this rhyme is
Keep well clear of Kingsley Amis.
Jim Thornton
Charity Function
This is from Louis de Bernières Imagining Alexandria (Click here). It’s straight sex that is on the way, but the poem is embarassing, sensual and kind, so still a fitting tribute to Cavafy.
Charity Function
She leaned across the table, confidentially,
As the dancers whirled to the cheap band
(For this was a charity function);
And drops of rain plashed aimlessly
Outside the marquee, whilst lovers retreated
From their kissing in the lilacs
And the rhododendrons.
She took the young man’s hand, toying with his fingers,
Glancing at the ham on paper plates
(For this was a charity function).
Then the rain drummed as the whole night shivered,
And nice old men in bow ties
Chatted to debutantes, and
Moths flared into the floodlights.
“Why don’t you come round for a chat sometime?
I’ve always got some beer.” She seemed forlorn,
And his heart leaped out, for
She was middle aged, no doubt her husband never touched her,
No doubt she didn’t want it;
But she was strong and hale, silent and suffering, and
Someone ought to love her.
He leaned across the table confidentially.
“I’d like that,”and it was no lie. It was
Not a charity function.
He was curious and amused.
Curious and excited, for
What could this be like?
And he was touched that he was trusted, that
It was him she asked.
It was him and not another.
Louis de Bernières
Top 10 of 2013
Ripe-tomato.org’s ten most popular posts of last year
Three circumcision posts (Cock-ups, Boston, Safer) in the top ten is to be expected. After porn, circumcision is the internet’s top topic! Three critiques of dubious science (Snoring, Alzheimers and Midwifery), an art scandal (Pollock), a sex scandal (Family Affairs), and a trip up the world’s tallest building (Cocktail).
Interpretations of Job
Misery by Joan Acocella
Last week’s New Yorker review by Joan Acocella of Mark Larrimore’s Book of Job: a biography (click here), begins with plot summary – Satan persuading God to test Job, first by harming his family and then Job himself, Job steadfast even after his comforters suggest he deserved it, until God appears in the whirlwind to tick them all off, punish the comforters and reward Job for repenting.
Over the last couple of thousand years pundits have tried to explain how God can so brazenly allow the innocent to suffer and the wicked to triumph. Perhaps Job’s problems presage the sufferings of the Jews, or of Jesus, or perhaps a higher justice is hidden from humans? Perhaps there is no God? Larrimore lists the theories, but Acocella concentrates on one. The possibility, raised by holocaust survivor Elie Wiesel, that the book is incomplete – it is certainly made up of different fragments – and that the ending is lost. Perhaps, Wiesel suggested, Job did not meekly defer to God. Maybe he just pretended to, or maybe he resisted. Or maybe he just went silent, realising that God was ultimately as impotent as man.
Whatever, says Acocella; only a discovery of lost scrolls will answer that question. But why does this book, of all the ones of the Old Testament, so fascinate us? The reason, she says, is the depiction of God. Job is just the pretext, “the one who is like us, and makes the argument that we would make”.
God is the one who speaks to us vividly. Where wast thou when I laid the foundations of the earth? When the morning stars sang together, and all the sons of God shouted for joy? When I created the animals: the goats, the asses, the hinds, the peacocks, the ostriches, the grasshoppers? When I created the eagle who dwelleth and abideth on the rock, upon the crag of the rock, and the strong place. From thence she seeketh the prey, and her eyes behold afar off. How dare you question me?
God as force of nature. Powerful, but not powerful enough to protect the innocent. As Acocella ends the essay: God bypasses all the moral “what should be” rest of the book of Job, and cuts to the real world. We may not like it, but “he makes the argument that, at least as far as nature is concerned, is true”.
Jim Thornton
Undercover surgeon
Heroic Platitudes

Ara Darzi, professor of surgery at St Mary’s, has incredible energy. He teaches medical students, trains surgeons, publishes prolifically (782 articles on Pubmed, 931 on his home page here), and still finds time to advise governments and sit in the House of Lords. This week he contributes Undercover surgeon (click here), the story of his night shift as a porter in his own hospital, to the BMJ Christmas issue. The cover features Darzi, standing on a blue whale!
But it’s dreadful writing. Removing the platitudes and clichés alone would cut it by half. “It was an eventful shift and not one I will forget in a hurry.” He mangles a colleague’s joke: Ara, there’s a porter operating on your patients, and … he’s not that bad!
His stories have no point. The one about being ticked of by a nurse for not warning her he was bringing a vomiting patient to the ward ends: “Throughout this quite extended telling off – and to the credit of neither of us – the patient remained unamused and feeling quite ill on the bed next to us.” He goes on: “I’m sure this example will not be new or shocking to many clinical staff, but it serves to emphasise the unintended yet detrimental effect on patients and their experiences that failed teamwork and interdisciplinary conflict can have.” Did he deliver his copy too late for sub-editing, or did no-one have the nerve to correct him?
But one story shines through – the surgeon as hero. Darzi takes all his ticking’s off in good part, runs the samples for a patient with internal bleeding to the lab, and finally knocks off at 3 am. At six he’s woken and called in to operate on the very patient whose tubes he had deposited earlier!
Did he do the stunt when he was already on call? Who cares? Even Lord Darzi, who runs a large department, does more research than six normal professors, and advises prime ministers, still gets called from his bed at weekends.
Thank heavens he can’t write.
Jim Thornton
Risk compensation after male circumcision
Conclusion contradicts data
This qualitative study of 28 recently circumcised Kenyan men, and another 18 awaiting circumcision, appeared in Health Education Research last week (click here).
As the authors admit, the design was inappropriate, and the samples too small and unrepresentative, to measure the rate of anything so, correctly for a qualitative study, they reported no numbers. Instead their aim was to tease out the existence of beliefs and behaviours which might have been missed in larger surveys, using in depth interviews and representative quotations. They were interested in whether men realised that circumcision only provided partial protection against HIV infection, and whether they were likely to increase sexually risky behaviour as a result.
For the first question it turned out that all respondents knew that circumcision provided only partial protection against HIV transmission. The authors concluded accurately that “Participants demonstrated good understanding of partial protection”.
But when they turned to risk compensation, namely whether respondents had used condoms less frequently or had more sexual partners after circumcision, they found the latter reported. Here is the relevant section:
“Only a few men said they would decrease their HIV protective behaviours after VMMC. Circumcised men spoke about sex being more pleasurable following male circumcision; as a result, a few circumcised men indicated they have sex more often (with their current partners) or have added another partner. At least one circumcised man said that prior to VMMC, sex and condom use was painful, but following circumcision he has more sex partners but has also increased his condom use because he does not feel pain anymore.
Two men were quoted:
Pleasure. Now sex is more sweet and enjoyable, so I said let me try another one again and even my former lady came back and I had sex with her. (Circumcised man, Kisumu East, age 27)
Since I got circumcised, I don’t feel pain while having sex and I feel the urge to add more [partners] … . I used to have sex without a condom because I was feeling pain … if I added a condom … but now I am using a condom because I no longer feel pain. (Circumcised man, Kisumu East, recruited into 18–24-year-old age group)
i.e. at least two separate men described actual “my former lady came back” or potential “I feel the urge to add more partners” risk compensation. The use of the expressions “a few” and “at least one” suggests that the actual number was higher.
Of course this tells us nothing about the rate of such behaviour, just that it exists. But in a qualitative study it should be reported as a positive finding. Instead the authors conclude:
“[…] there was little suggestion of risk compensation following VMMC.”
This is blatant misrepresentation. The correct interpretation is that both potential and actual risk compensation was reported. Further studies are required to measure how frequent and relevant this is.
Readers must assume that the authors, social scientists from Research Triangle Park in North Carolina, rather than being disinterested seekers after truth, are biased advocates of voluntary male circumcision. Can we be sure that the interviews were conducted and transcribed in unbiased fashion?
Jim Thornton
Labiaplasty
Never on the NHS, and never ever on the young
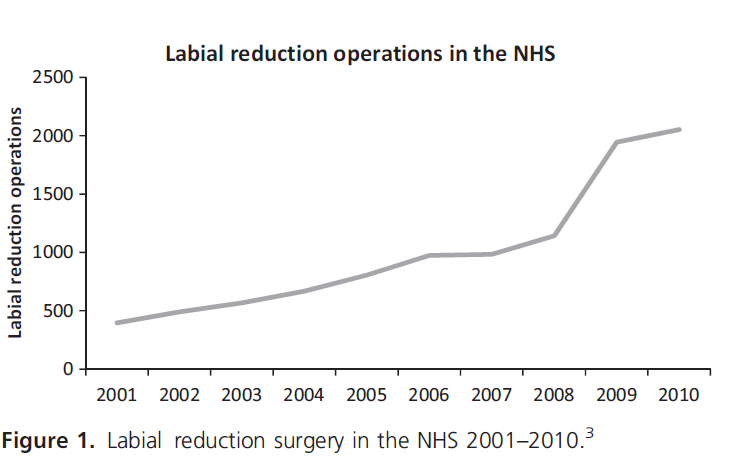
The motion; Labiaplasty is a form of genital mutilation and should be banned was carried, just, by an audience of trainee gynaecologists in Nottingham last week (click here). Phew! There is an epidemic of this sort of surgery (figure) and it’s time it ended.
For every NHS operation, there are dozens of private ones. A recent study (click here) confirmed what any experienced gynaecologist knows; a mix of sexual and psychological insecurity, typically provoked by mother or boyfriend saying “that’s not right” underlie most requests. Folk memories that other ethnic groups have large labia, that enlargement is a sign of excessive masturbation, or desires for a pre-pubertal state remain unspoken, leaving claims of physical discomfort to justify surgery. Demand bears little relation to anatomical variation (see for example the Great Wall of Vagina here). Poorly documented claims by surgeons fill the scientific literature, while patient tales of cures, botched operations, and ongoing distress fill the internet.
Despite my debate victory, I doubt a ban is justified. We should protect children and the vulnerable from irreversible surgery, but adults do all sorts of things to their bodies in the name of sex. Good luck to them. It’s just not something for the NHS. Two recent reports agree. The Royal College of Obstetricians and Gynaecologists (RCOG click here) said in October 2013:
“[…] providing labiaplasty for cosmetic reasons alone is not a proper use of public resources and should not
be provided by the NHS.”
and the Society for Paediatric and Adolescent Gynaecology (SPAG click here) said:
“Labiaplasty does not tackle the cultural and economic factors that are giving rise to vulval appearance distress. There is no scientific evidence to support the practice […]” and “[…] labiaplasty should not be performed on girls under the age of 18 years.”
Well said.
Jim Thornton
Screening Old Men for Abdominal Aortic Aneurysm
Not worth it
Ruptured abdominal aortic aneurysms (AAA) rarely end well. But ultrasound scans can detect them before they pop, and elective repair has 95% survival, so they may justify screening. On the other hand surgery is expensive, especially on the sort of overweight smokers who are at most risk of AAA, they don’t all burst, and keeping a watch on the borderlines stresses people out, so screening might do more harm than good. Fortunately we have evidence.
Three large randomised controlled trials have conclusively shown, at least for men aged over 65, that screening saves lives (click here). About 200 men need to be scanned for each life saved, at a net cost according to the NHS experts of about £100 per man screened or £7,600 per additional year of life in full health – Quality Adjusted Life Year or QALY in the jargon. This is better value for money than many other NHS treatments (details here). In about six years I’ll get an invitation. What’s not to like?
The trouble is the cost benefit analysis is flaky. A recent paper (click here) found seven economic models of AAA screening all based on the same trial evidence. The cost per QALY varied from €4,000, in an analysis from the UK (click here) to €57,000 per QALY in one from Denmark (click here). The review authors reckoned the differences were due to different assumptions within each model, which outside observers cannot easily judge as correct or not. I can’t contribute to that sort of technical discussion, but I can see one big flaw in those models I can understand.
None of the models include the cost of success. Ruptured aortic aneurysm is usually a quick way to go. About half simply drop dead, and at least half the rest die after a few days in hospital. If this quick death is prevented by screening, the patient still has to die of something. Since most deaths are slow, it’s likely to be more expensive, much more if it’s Alzheimers. Even the successfully treated man who lives into his 90’s is spending his pension, rather than generating wealth. Once we stop working we cost less dead. If I’m right all the models underestimate the costs substantially.
There’s another reason to doubt the lower cost estimates – why isn’t there a free market AAA screening programme aimed at moderately wealthy old geezers? £100 per man screened is not much for a person on even a modest pension. Plenty of countries with rich people in them don’t have state-funded screening programmes. If the net cost was really £100 per punter there should be money to be made offering scan/operation packages. Nowhere in the world are private practitioners offering AAA screening to the uninsured for £100 a pop – excuse the pun – or anything like it.
Lack of a private service should give the NHS cause for thought. If no middle class men anywhere, fork out for AAA screening, why should we believe some economist who is essentially saying they they don’t know what’s good for them.
But perhaps I’m wrong. Maybe it really is as cheap as the health economists say. I still object to paying for it.
Whatever happened to the idea of deserving and undeserving patients. It may be politically unacceptable to say that some people deserve health care more than others, but it doesn’t make it less true. I’d rather spend money on a cancer treatment for teenagers that cost £20,000 per QALY, than on AAA screening at £7,600 per QALY. A year of life at 20 is worth more than one at 70, and if you’re struck down through no fault of your own, you’re more deserving than an old geezer who’s been smoking, boozing and overeating half his life.
Jim Thornton
Larkin’s animal poems – 7
Late Larkin
Larkin had told many friends about feeding the hedgehog in his garden and was devastated when he accidently killed it. But note the “twice” in line 1, an unsentimental Larkin detail. Without realising what was happening, he had restarted the motor and finished it off.
Aside from scraps composed for retirements and anniversaries, this is the last poem he wrote. I’m glad that his final poetic comment on death was not the terrifying Aubade but these tender thoughts on a hedgehog.
The Mower
The mower stalled, twice; kneeling, I found
A hedgehog jammed up against the blades,
Killed. It had been in the long grass.
I had seen it before, and even fed it, once.
Now I had mauled its unobtrusive world
Unmendably. Burial was no help:
Next morning I got up and it did not.
The first day after a death, the new absence
Is always the same; we should be careful
Of each other, we should be kind
While there is still time.
Philip Larkin
See also Take One Home for the Kiddies here, At Grass here, Myxomatosis here, First Sight here, Pigeons here, and Laboratory Monkeys here.
