Standard, Population & Customised fetal growth charts 14 – GROW
Customised charts
The Perinatal Institute (click here) is a leading UK advocate of customisation. It markets Gestation Related Optimal Weight (GROW) charts, customised on the mother’s height, weight, ethnicity and parity (1). Two charts are typically combined into one physical chart which can be printed out and filed in the woman’s record. The left hand scale shows fundal height in cm and the right hand estimated fetal weight (EFW) calculated from a combination of biparietal diameter, head circumference, abdominal circumference and femur length, using Hadlock’s formula, in grams. Staff are encouraged to plot fundal height using an X symbol and EFW using a O. Examples below.


The left hand chart is for a normal weight and height British European woman (2), and the right for an underweight Indian woman. Both customised charts include an estimate called the Term Optimal Weight (TOW). For the British European baby this is 3,429g and for the Indian one 3,042g. The difference matters. Imagine that the EFW was 2,000g at 39 weeks. The British European mother would be told that her baby was growth restricted and likely advised to have labour induced, but the Indian woman would be told that the weight was “normal for her ethnicity, height and weight” and probably allowed to let the pregnancy continue.
Their customisation principles are detailed on the website (click here) but the exact formulae in use at any one time are a commercial secret. They are regularly updated on the basis of data sent back to the Institute by their customers. This is a potential weakness since, although GROW customers have been trained in both fundal height and scan measurements, it is unlikely that the biases which inevitably affect revealed human measures in practice will have all been removed (click here).
The underlying justification for the choice of features on which GROW charts are customised is also weak. Self-reported ethnicity has both theoretical (click here) and practical (click here) problems. Maternal height (click here), weight (click here) or parity (click here) are problematic because underweight, shorter, and first time mothers all have both smaller babies and higher perinatal mortality. Customisation on those features thus risks normalising pathology. It would only be justified if we could be sure that the strength of relation between each feature and adverse outcomes was weaker than that between birth weight and adverse outcomes (click here). There are no such data. Even those WHO standard chart authors who advocate customisation in theory, have not even attempted to provide such data (click here). Customisation by fetal gender makes theoretical sense (click here) but GROW charts do not at present offer this.
Finally GROW only provides customised charts for fetal weight, not for head or abdominal size, or fetal length separately. This condemns obstetricians using GROW charts to either ignore these component measures or to interpret them on a different, non-customised chart (click here).
The Institute’s director, Professor Jason Gardosi, claims that GROW chart introduction was associated with a reduction in stillbirth and that the reduction was greater in English regions with higher uptake of GROW charts. Both claims are doubtful. The following are screen grabs taken from a lecture he regularly gives, available on the Institute’s website (click here). The data are those in his BMJ Open paper (click here). The graph scales appear to have been selected to emphasise a point.


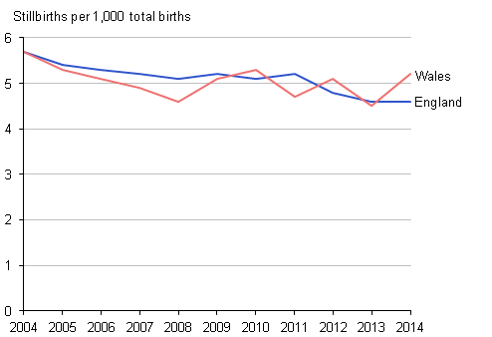
Note how the vertical scale differs between the left and middle slide. The right hand slide (3) is fairer. Stillbirths were falling long before GROW charts were introduced and if anything the trend has levelled off.
The choice of time periods and regions to report may also be selective. See left and middle figures below.

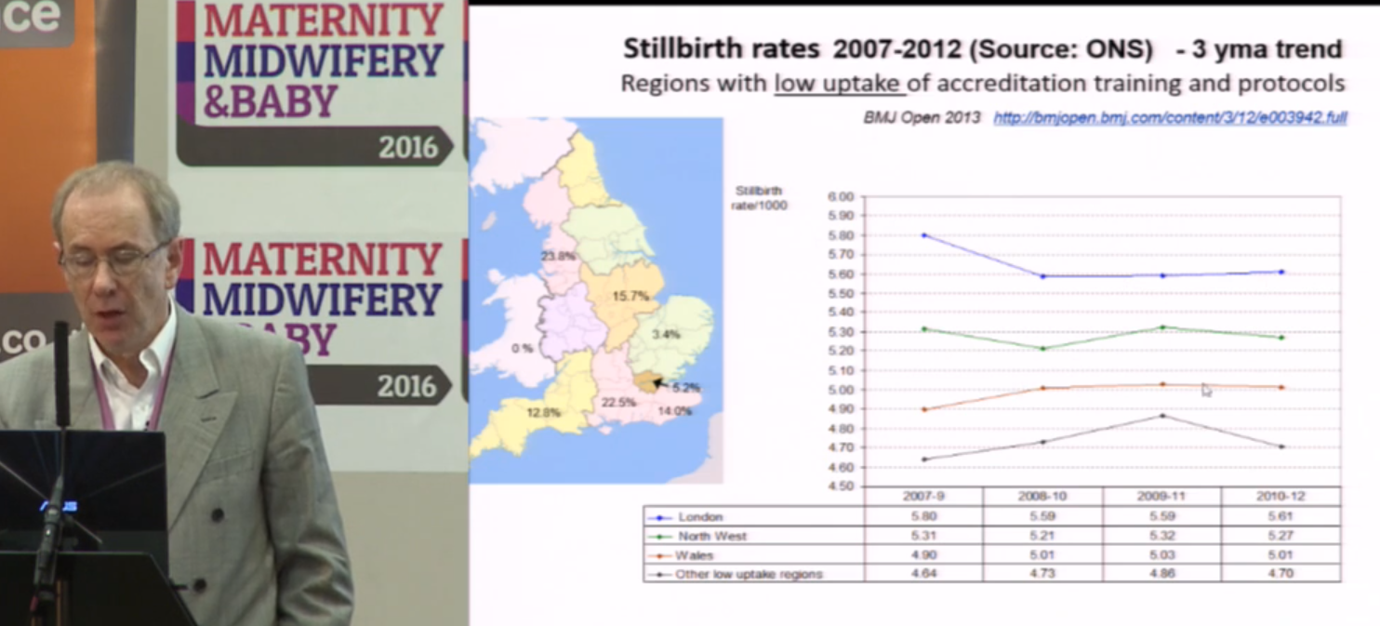

The right hand slide shows the same data for the whole of the UK (3). The rate of fall slowed slightly in England and Wales where GROW software was most widely used, and was steepest in Scotland where GROW software was not in use.
The reasons for this general trend are well understood. Falls in smoking, increased diagnosis and termination for lethal fetal abnormalities, and increased inductions near term, all three of which reduce stillbirths. Given the undoubted benefits of the rest of The Perinatal Institute’s training in encouraging staff to measure fundal height correctly and to act on the results, this hardly suggests that customisation is beneficial.
Next, other empirical comparisons (click here)
Jim Thornton
Footnotes:
- The Perinatal Institute also provides training in various aspects of maternity care. This latter work is generally agreed to be excellent.
- British European is not currently one of the official UK ethnicity groups. Presumably the Perinatal Institute authors mean White British.
- I thank Professor Gordon Smith for the national stillbirth data.

Trackbacks