Jim’s tweet
Home birth after three Caesareans
A few days ago I tweeted:
The link (click here) was to a mother’s post about her successful home vaginal birth after three Caesareans (HVBA3C). The recipients were James Titcombe whose son Joshua died in Morecambe Bay NHS Trust, led the campaign for a public enquiry, and was vindicated by the Kirkup Report (click here). Amy Tuteur is a retired US obstetrician and blogger who campaigns against, as she sees it, anti-science attitudes in pregnancy and childcare. Her views on anti-vax parents are mainstream, but her rejection of the idea that natural childbirth is a good in itself, and specifically her uncompromising hostility to home birth, (click here for her blog) get some people’s backs up.
Sheena Byrom, a retired UK midwife, and author of many books about natural childbirth tweeted; “I am so shocked that you engage this way on Twitter Jim. Is it a game?”

Byrom had crossed swords with Tuteur before – she regards her as an internet troll who enjoys picking fights with supporters of natural childbirth – and felt it inappropriate to copy a mother’s personal, albeit public, blog about her happy and successful birth to such a person. James Titcombe defended me, and soon found himself embroiled in the row. Others accused me of being unprofessional, and likened Titcombe, Tuteur and Thornton to Macbeth’s three witches.
Before long Tuteur had lived up to Byrom’s expectations by fanning the flames as hard as she could (click here and here). Tuteur has a pungent writing style – I’m sure neutrals find her a good read, and you wouldn’t have to look hard to find health professionals who agree with her – but she does go for the woman not the ball!
I’m afraid I kept my head down – accusations of unprofessionalism, especially when copied to the RCOG make me nervous; I’m still in clinical practice and have had run-ins with them before – and when something goes viral it is difficult to avoid digging a bigger hole. But the argument and retweeting have gone on and on. So here are my thoughts.
Background
My initial tweet was not out of the blue; I don’t search the internet for risky birth stories to show Amy Tuteur. It followed an invitation to comment on another mother’s blog (click here) describing her successful vaginal birth after two Caesareans (VBA2C).

Like the anonymous obstetrician criticised in that blog, I strongly discourage VBA2C, but the references cited, and RCOG guidance suggest I may be wrong, and I’ve also reluctantly looked after a couple of cases myself, which I admit turned out OK. So I said what I usually say, “discourage but support”.
Soon I was invited to comment on another post. The one whose link I later forwarded, namely the home vaginal birth after three Caesareans (HVBA3C).

Calling HVBA3C a “first world problem” was flippant, but I still think that home birth in that situation was foolhardy. The risk of uterine rupture is at least 1 in 200, perhaps higher without continuous fetal heart rate monitoring, or if the woman is determined to push on in the presence of slow progress, and the baby will certainly die if rupture occurs at home. It’s not as dangerous as Russian roulette, but considerably more so than not buckling yourself or your baby into your car seats. So rightly or wrongly, I forwarded the link to Titcombe and Tuteur.
Why did it cause such trouble?
There is a battle here, and some truth on both sides. Modern obstetrics, the stuff I do every day, is obsessed by reducing risk. Caesareans for breeches, antibiotics for positive group B strep swabs, and heparin for anyone with a risk factor for thromboembolism are all unnecessary most of the time, but heaven preserve the doctor who skips them if a bad outcome occurs. We drill our staff again and again about how to interpret fetal heart rate abnormalities, and even then we don’t trust them completely; every few hours we insist on a “fresh eyes” review. We’re trying to squeeze the last drop of risk out of childbirth, and that’s not a bad thing. Parents want a healthy baby. They don’t want to hear:
“We’re sorry things turned out bad, but your complication is rare. To prevent your baby’s death we’d have to monitor hundreds of babies, do hundreds of Caesareans, or give thousands of women antibiotics.”
They would rightly reply:
“Why not? I’d have a Caesarean for a 1 in 200 risk, or take penicillin for a 1 in 1000 one.”
But our obsession with safety has a cost. It causes anxiety. Fetal monitoring does lead to unnecessary Caesareans. People popping in and out of rooms to review progress, give antibiotics and check heart beats, stops women relaxing and may actually slow labour.
And supporters of natural childbirth are right. Hospitals are not perfect. Too many women still labour on their backs. Doctors make stupid decisions. And even if we were perfect, it might still sometimes be better to take a bit of risk to allow nature to take its course. Homebirth might be less risky than we believe.
The Birthplace Study (click here), undoubtedly the best quality research into the question, showed that for low risk multiparous women, looked after by properly trained midwives in the UK, home is as safe as hospital. Even for first pregnancies the additional risk is quite small, such that some women might rationally decide to take it. I’m not an opponent of home birth.
But, there surely is a line we should not support, and birth at home after Caesarean is on the wrong side of it. We can’t stop parents making bad decisions, but professional supporters of home birth unavoidably tread that line. Read the HVBA3C story again (click here). Did the midwife who told the mother she could have “a natural birth no matter how many sections I’d had” cross it?
Last year, the Kirkup report on Morecambe Bay concluded:
“Midwifery care became strongly influenced by a small number of dominant midwives whose ‘over-zealous’ pursuit of natural childbirth ‘at any cost’ led at times to unsafe care.”
When I read that at the time, my reaction was: Surely not. I’ve never met or, until Kirkup, even heard of a midwife acting like that. Lots of other things went wrong in Morecambe Bay, but this sounds like someone is dumping on the midwives.
And I’ve read Sheena Byrom’s writings, and I know people who know her well. She is not “pursuing natural childbirth at any cost”. At the risk of putting words in her mouth, she would say that once a woman has decided to have a home birth whatever the risk, typically after being told ad nauseam by people like me and Amy Tuteur that she is risking her own and her baby’s life, there is nothing to be gained and everything to be lost by banging on about the dangers again. We cannot arrest women. If they fall out with their home birth midwife, they don’t always return meekly to hospital. They sometime deliver at home with no assistance at all. That is much less likely to end well. I get all that.
So let me be plain. Amy Tuteur is wrong. Sheena Byrom and her colleagues are also trying to make birth safer. I am sorry my tweet led to their motives being impugned yet again.
But …
When one of the retweeters wrote about the HVBA3C blog “What an amazing story thanks for sharing let’s hope it empowers more women”, I did have sympathy with Amy Tuteur’s response:
“Let’s hope it doesn’t kill anyone”.
Midwifery and obstetrics are tough jobs. We tread narrow lines.
Jim Thornton
Late published trials
Public sector worst offenders
The pharmaceutical industry is often accused of failing to publish their clinical trials; a paper in this week’s New England Journal of Medicine confirms they are sometimes guilty, but far from the worst offenders. Click here for full text, or for those with access problems, rct results reporting.
Among 32,656 trials, registered at ClinicalTrials.gov, and completed or closed by August 2012, only 13% had reported within one year, and 40% by four. Commercially funded trials were significantly more timely than those funded by government, academia or charities. Here’s the graph.
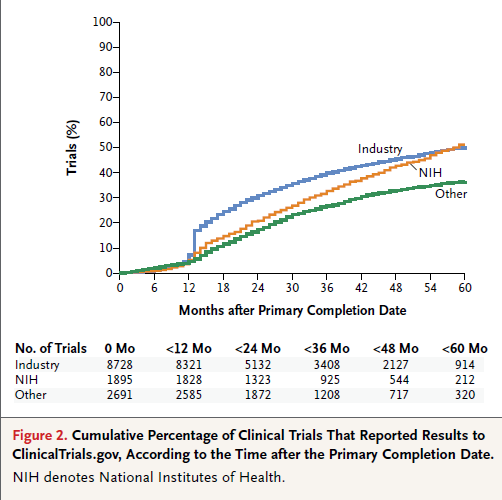
The researchers also checked if they had a good reason for delay. Nearly half of industry trials (44%) did, compared with only 6% of NIH funded ones and 9% funded by other sources. Overall industry reported 80% of trials on time, or had an acceptable reason for delay, as compared with 50% NIH trials, and 45% for those funded by others.
Even these results are probably biased in favour of the public sector. Industry must register its trials to use the results for licensing. Trials funded from other sources, often delay registration till publication; check submission and registration dates if you don’t believe me.
Click here, here, here or here for a few egregious examples of late registration or other registry cheating in public sector trials.
Time to stop beating up pharma?
Jim Thornton
Lesbian reaction shot?
Sappho’s Fragment 31
We don’t know the sexuality of the 7th century BC poet who gave her name to Sapphic love – the Greek verb “to act like someone from Lesbos” originally meant “to be a sex mad predator of men” – but fragment 31 about love between women, remains one of her most erotic poems. It is in the Sapphic metre of three long lines followed by a fourth short one, and maddeningly is missing its ending. Daniel Mendelsohn’s translation is from this week’s New Yorker.
The poet never describes the object of her affections directly; instead envy of the man talking to her lover is followed by her own emotional and physical collapse in the loved one’s presence. As Mendelsohn puts it, the poem is “a kind of reaction shot”.
He seems to me an equal of the Gods—
whoever gets to sit across from you
and listen to the sound of your sweet speech
so close to him,
to your beguiling laughter: O it makes my
panicked heart go fluttering in my chest,
for the moment I catch sight of you there’s no
speech left in me,
but tongue gags—: all at once a faint
fever courses down beneath the skin,
eyes no longer capable of sight, a thrum-
ming in the ears,
and sweat drips down my body, and the shakes
lay siege to me all over, and I’m greener
than grass, I’m just a little short of dying,
I seem to me,
but all must be endured, since even a pauper …
Obstetric FGM prosecution
Whose fault?
Many blame Alison Saunders, the director of public prosecutions (DPP), for last week’s ill-advised prosecution of Dr Dharmasena on the charge of performing female genital mutilation (FGM) during repair of a previously circumcised woman’s vagina after childbirth. I confess I did at first (click here). They accuse her of trumping up a charge to cover her failure to prosecute any primary cases, and contrast the delay in bringing this flimsy case to court, with the 25 minutes the jury took to throw it out.
Dr Katrina Erskine, a consultant OBGYN at Homerton Hospital, with considerable experience in treating victims (here):
“It is ludicrous to conflate anything a doctor or midwife may do at the time of delivery to a woman who has already suffered FGM with FGM itself, and it is insulting to women who have actually suffered FGM. […] It is also a diversion from what we should really be addressing, which is to try and find a way to reduce the incidence not just for girls born in the UK but worldwide.” The decision to prosecute has ‘left me with no faith in British justice’.
The president of the Royal College of Obstretricians & Gynaecologists (RCOG) writing to members and fellows yesterday (David Richmond’s letter):
“[…] this was the wrong prosecution at the wrong time of the wrong individual. It has generated an enormous degree of anger at the process, sympathy for the patient and concern for the trainee involved. It is difficult to understand how a case that took a year to bring to court was so flimsy that it took the jury less than 30 minutes to dismiss.”
But lawyers aren’t experts in FGM. This particular DPP is a woman, but she’s just a lawyer, advised by medical experts, and campaigners. It is the latter who over reached. Most have been rather quiet, but one put her head above the parapet, Lib Dem MP, Lynne Featherstone (click here):
‘Whatever the outcome of that case, the shock waves sent through the medical profession when the arrest was announced, hopefully will be very significant in making everyone in the frontline think, what am I doing? Do I know about this?’
In other words, FGM is a terrible crime and we need to publicise it to end it, so let’s prosecute an obstetrician from time to time “pour encourager les autres”.
Imagine what Lynne Featherstone would have said had Alison Saunders declined to prosecute Dr Dharmasena, and a garbled version of events had got into the public domain. The DPP was damned whatever she did.
Featherstone is typical of a certain sort of campaigner. FGM is bad, so every possible form of it is bad. Primary infibulation is a crime so re-infibulation should also be a crime. It’s understandable; no-one wants any woman to be re-infibulated against her will. But it’s hardly the main problem. As we learned last week, at least partial re-infibulation might be needed medically, and if requested by an adult women is not a million miles away from cosmetic vaginal surgery.
Other campaigners have persuaded the World Health Organisation (WHO) to include any genital piercing, or pricking with a needle, within the definition of FGM. It’s sort of logical, but it’s not common sense. When some Malaysian parent gets prosecuted for doing a tiny needle prick, perhaps to avoid their daughter getting something worse, will we still blame the DPP?
Many campaigners are understandably annoyed when men draw parallels with newborn male circumcision. They can clearly see that although that is wrong, it’s an order of magnitude less wrong and more nuanced than FGM. Why can’t they see that reinfibulation, or pricking with a needle are also wrong, but an order of magnitude less wrong and more nuanced than primary clitoral excision?
This whole trial was a mess, and should never have happened. But don’t blame the lawyers. The doctors, midwives, and paediatricians who advise them, and the campaigners who cheer them on, should look to themselves. FGM is a terrible thing. We should fight the real thing.
Jim Thornton
Well-cooked CHIPS
Control of Hypertension in Pregnancy Study
High blood pressure (BP) in pregnancy carries risks for both mother and baby, but for years doctors have been treating it without knowing what target BP to aim for. Everyone agrees with lower than 160/110 to prevent maternal stroke, but they worry about getting near normal (120/80) for fear of reducing placental blood flow and harming the baby.
Such concerns were justified by both theoretical arguments and some rather poor quality trials, but in this week’s New Engl J Med (click here or CHIPS Trial – NEJM 2015), Laura Magee and her colleagues from Canada, show they were misplaced.
The CHIPS trial compared less tight control (target diastolic 100) with tight control (target 85). It was registered here in 2008, with a planned sample size of 1028. They recruited 1030 women, but on the advice of the independent steering committee, excluded 43 women from one site due to concerns about data integrity and consent, leaving 987 for analysis. The odds ratio of the predefined primary composite outcome (fetal loss or >48 hours neonatal intensive care) with less tight control, was 1.02; 95% CI 0.77-1.35. In other words there were no fetal risks from aiming for a target diastolic of 85.
Since lower is clearly better for the mother*, we should now aim for tight control. I’m changing my policy today, and the National Institute for Clinical Excellence (NICE) will surely soon amend its advice.
Robin Hood’s contribution
I’m also proud. Nottingham University Hospitals NHS Trust sponsored the UK arm. Dozens of UK doctors and midwives (listed here), supported by the UK National Institutes of Health Research, patiently explained the uncertainty to pregnant women and their partners, recruited those who wished to participate, and followed everyone up. The UK was the highest recruiting country worldwide.
Next steps
There is a rumour that the US National Institutes of Health (NIH) have just funded pretty much a repeat of the CHIPS trial. Some colleagues blame the “not discovered here” syndrome, but I think that’s unfair. Even after randomising nearly 1000 women the confidence intervals around the fetal effect in CHIPS is compatible with a 20% reduction and a 30% increase in bad outcomes with less tight control. Millions of women have hypertension treated in pregnancy every year. A repeat trial to narrow these confidence intervals is worthwhile.
I’m following a “tight control” policy, but I’ll be looking out for the US trial results.
Jim Thornton
*CHIPS didn’t prove that. Although the primary adverse maternal outcome was higher in the “less tight” group, the difference (3.7 v 2.0%) was not statistically significant. I doubt any feasible pregnancy trial could prove maternal harm, because bad maternal outcomes are rare. But many observational studies have shown that very high BP is associated with maternal strokes, and the rate of dangerously high BP (>160/110) was greater in the “less tight” group.
The UK’s first FGM prosecution
Second guessing the DPP
The extraordinary trial of Dr Dharmasena, the obstetric registrar, who repaired a woman’s vagina after childbirth and now finds himself accused of performing female genital mutilation (FGM), has started (click here).
The case, as presented by the director of public prosecutions (DPP) last year, made so little sense that informed commentators (click here) assumed a political motivation, and that it would either be quietly dropped or that some new detail would emerge to justify prosecution.
Perhaps the prosecutor would bring the victim to the stand to tell the court how she had begged Dr D to leave her labia unsutured, and he had said something like: “No. Your husband wants a wife with adherent labia, so I’m going to re-suture them closed.” I doubt this is the DPP’s case because we are told the alleged victim has not even made a statement. If it were, it would indeed be terrible medicine, but not FGM; operating without patient consent is assault.
Or perhaps Dr D and the husband had colluded to remove more tissue during the re-suturing. But nothing like that is alleged in the prosecution’s case, at least as summarised in the Guardian (click here).
It appears that, either at her request, her husband’s request, or at her request through her husband, or to stop bleeding, or because he thought that was what everyone else did, or as a result of some combination of these reasons, (Dr D is alleged to have changed his story) Dr D restored the anatomy the patient came in with. He couldn’t restore it to her birth state, because the labia and clitoris had been thrown away somewhere in Somalia, but the prosecutor seems to think he should have got a bit nearer to that ideal.
I confess I’ve missed the law about restoring anatomy. What would such a law say if the woman had become accustomed to her post FGM anatomy, and asked to stick with what she knew? Perhaps the midwife, Aimma Ali, who is said to have objected to Dr D resuturing the labia at all, will shed some light.
It’s tough being an obstetrician. We not only have to keep parents and family onside – everyone’s an expert in how to deliver babies – and to make every decision with half an eye on the civil courts if a bad outcome ensues, but now we also have to second guess the DPP’s idea of an acceptable anatomical result.
Jim Thornton
Fragrance of Mercy
Rose Distribution
Today members and supporters of the Khalifa Qamar Zaman (KQZ) Legacy Institute (click here) met by the Brian Clough statue in Nottingham’s Market Square to commemorate The Prophet’s birth.



The speakers were Imam Khalid Hussain from Leicester, and Paddy Tipping, Nottinghamshire’s Police Commissioner. In the aftermath of the Paris shootings at the offices of Charli Hebdo and at the Hyper Cacher Jewish supermarket, the distribution of roses and the messages of peace and tolerance had special importance.
#JeSuisCharlie






This’ll turn you feminist
The effect 0f male circumcision on female HIV infection – the evidence
If it becomes obvious mid-way through a randomised trial that a new treatment doesn’t work sufficiently well to make it worth using, stopping early is good practice; we may never get a clear answer, but who cares? But if you’re planning on using the new treatment anyway, you really must finish the trial, and sort out once and for all whether it does harm.
Consider a treatment which affects husbands and wives. Treating one automatically treats the other. Evidence accumulates that it is good for the husband but results are unclear for the wife. It would be bonkers to stop when interim data showed a non-significant harmful trend for wives, on the grounds that the treatment was never going to be good for them, and then go ahead and implement it! But that’s what the authors of the only trial ever to test the effect of male circumcision on HIV transmission to the woman did (click here).
They tested the hypothesis that circumcision of HIV positive men would reduce new cases of HIV in female partners, as part of a larger trial including HIV negative men. When the HIV negative cohort closed, the investigators fretted that “continuation […] in HIV-infected men could result in stigmatization” and “determined that the conditional power to detect 60% efficacy, […] was only 4.9% and recommended that enrolment be closed.”
At that point 17/93 (18%) intervention and 8/70 (11%) control women had become infected. The difference might have occurred by chance (hazard ratio 1.58, 95% CI: 0.68–3.66, p=0.287), but if it was real, wives would surely want to know. The harmful effect is biologically plausible; the foreskin functions as a sleeve within which the penile shaft moves during intercourse to reduce vaginal and penile abrasions. But the trial stopped, and the US, WHO, and the many governments who get funds from those sources, went on to encourage male circumcision, without mentioning the possible increase in female infection risk. For the WHO fact sheet (click here).
Some circumcision advocates (e.g. here) admit that the evidence on male to female transmission is unclear, but conclude “that women will benefit from […] voluntary medical circumcision programmes in the long-term” on the basis of modelling studies like this one (click here).
But the modelling studies ignore even the possibility of increased male to female transmission. For the base case this one assumed 60% effectiveness for men, 80% coverage by 2015, and no post-circumcision behaviour change. They tested the effect of varying all these in a sensitivity analyses but not the effect of any increased male to female transmission. Am I going mad?
Let’s summarise. Randomised trials show that male circumcision reduces female to male HIV transmission by about 60%. The only trial which measured it showed a biologically plausible increase in male to female transmission of 58%, but was stopped before it gave a clear answer. Experts modelled the effect of their programmes assuming the male benefit was real, but ignoring even the possibility of increased male to female infection. On the basis of such models millions of men are circumcised, and millions of uninformed women are put at risk.
It’s enough to turn even me feminist!
Jim Thornton
Francesca Says More
By Olena Kalytiak Davis
In the 13th century Francesca da Rimini, stuck in an arranged marriage, shared the story of the knights Lancelot and Galehot’s love triangle with Queen Guinevere, with her husband’s brother Paolo. It struck a cord, and overcome by passion they began a ten-year affair. When her husband finally caught them at it, he murdered them both. In the Inferno Dante meets Francesca and Paolo in the second circle of hell, reserved for the lustful.
Davis calls this poem, one of a series about Francesca, a “shattered sonnet”, and includes it in her latest collection The Poem She Didn’t Write and Other Poems (click here).
that maiden thump was book on floor, but
does it really matter who kissed who
first or then who decided to go further?
lower? faster? naturally, we took
turns on top. now here, now there, and up
and down…once it started no one even thought to think to stop.
so, we have holes inside our souls,
but mustn’t we begin by filling others’?
god gave us lips and hands and parts
that cannot possibly be saved for prayer. nor by.
i will not name name, claim fame by how well
or who I fucked or why, it happens all the time.
and it’s you, white pilgrims, whom next galehot seeks.
fuck. we didn’t read again for weeks.
Olena Kalytiak Davis
Circumcision video
Often a vivid story or picture carries more weight than any amount of science or ethics. This blog received more hits for some pictures of circumcision complications (click here) than for any other post. Comments about flawed newborn tongue-tie cutting trials were ignored until I drew parallels with circumcision (click here).
This is why I’m publicising this video clip of a brit milah. There’s no blood, and we don’t see the surgery. Just a few off colour jokes, men chanting over the baby’s cries, and the women’s mixed feelings. It’s been posted by the baby. He wants you to watch. Click here.
