Irrational surgery
Cutting the lingual frenulum, or the uterosacral nerve “because it’s there”
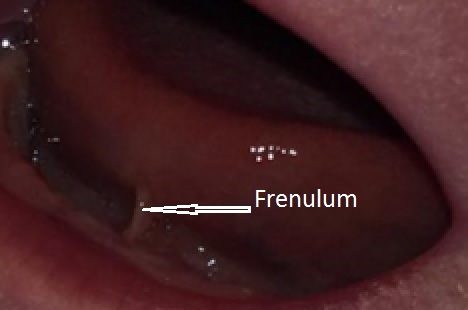
Frenotomy
Frenotomy to treat breast feeding problems makes little sense. Some people can stick their tongues out further than others but, apart from a tiny minority with other problems, the ability is unrelated to health. Even if it was, cutting the frenulum, the midline fold of skin which we all have under the tongue, is unlikely to alter function. The tongue is a big muscle; why would cutting a thin fold of skin in front of it matter? Orthopaedic surgeons don’t alter a muscle’s action by trimming round the edge, they remove it from its bony attachment and reattach it somewhere else. Even if the frenulum limited tongue movement, scars contract; cutting is just as likely to reduce mobility. You need z-plasties or similar to prevent contractures.
Empirical trials don’t support frenotomy either; most trials cut patients in the control groups within 48 hours so they could only measure the effect on very short term maternal pain (click here). The only trial which delayed cutting controls for two weeks was negative (click here). So why do up to 10% of babies get their “tongue ties” cut? Because it’s there.
Open the baby’s mouth and anyone can see it. Naive parents easily believe the story that it is limiting tongue movement. Cutting is easy, the baby can’t fight back, and complications are few. If the breast feeding problems resolve, the parents credit the operation. If they don’t, the surgeon can claim it was done too late, needs repeating, or doesn’t always work.
LUNA
Not so long ago laparoscopic uterosacral nerve ablation (LUNA) was the gynaecological equivalent of frenotomy for painful periods. Cutting the nerves to the uterus is not straightforward; an extensive plexus of nerve fibres lies deep in the retro-peritoneal space alongside the ureters and large arteries and veins. A proper nerve cutting operation, pre-sacral neurectomy, is difficult and risky; a last resort for women with disabling pain which can be treated in no other way. The results are modest at best.
But laparoscopy allows even ordinary surgeons to have a go. The uterosacral ligaments don’t contain many nerve fibres, but they need no fancy dissection to identify, and contain no important blood vessels.

Any surgeon who could clip a Fallopian tube could do LUNA. Poorly designed studies suggested it might work, and it became a common and lucrative operation. Since most pelvic pain resolves with time many patients were convinced they’d been cured, and some surgeons made good money. A few women had complications, but if it works … .
Eventually a group of researchers the LUNA Trial Collaboration, did a proper randomised trial – including a sham incision on controls, vital to avoid a placebo effect (click here or LUNA trial full report. Full disclosure – I was a participating surgeon).
Result – absolutely no effect from LUNA. Looking back it was obviously going to be so. There was no underlying logic. It was popular because it was there, and any old surgeon could do it. LUNA has pretty much died away from embarrassment.
Come on NHS. It’s time for one well-designed trial to send frenotomy the way of LUNA.
Jim Thornton

Dear colleague
would you be willing to publish this in the South African Journal of Medicine?
with best wishes
Daniel Sidler
[cid:dd179b33-39a1-4ad8-b066-8dd1fd628363]
________________________________
Delighted Daniel. I’ll email you. j
Very interesting article. I completely agree that someone has to step up and look at this matter in a well structured way. Thanks Prof!
Mr. Jim Thornton on L,U.N.A.,
As a reporter it would behoove you to contact the surgeon who invented L.U.N.A. 40-years ago to discover what was the feeling of women’s health care at that time and what was the scientific findings so long ago and what has happened since then.
Women in the late 1970’s were considered ‘complainers’ who would do anything to avoid sex, even though the ‘vaginal itch syndrome’ was identified to be trichomoniasis and Ponstel(R) a drug like ibuprofen was effective for some women’s pain. I took a desperate woman who had seen more than 10 doctors for incapacitating pain 7 days per month to the operating room and burned and transected her utero-sacral ligaments because another researcher had reported that biopsies confirmed the virus herpes could be found in these uterosacral nerves. Jodi remained pain free for 30 year and is now in menopause. A panel of pain specialists and gynecologists convened to review my request for a double-blind study (one active and one sham). I did the surgery and another doctor and the chairman’s secretary confirmed the findings. For the first 3 months, 10 of 11 were pain free. There was no dilatation of the cervix to confound the findings. All 10 in the control group did not find relief. THE PURPOSE of the study was to confirm that the pain was real for these women. At 6 month intervals they were polled and the effectiveness of the surgery dropped as I expected the nerves ‘grew back’. I stopped my office to measure the pressure in the uterus in a woman scheduled for surgery — the pressure catheters confirm that the uterine pressure was 400mmHg which is four times greater than necessary to deliver a baby. The pain occurred because the cervix muscles closed down the opening (os). When lidocaine was injected into the cervix, the cervix relaxed first and then the uterus thereafter. Again, proving the pain was real and there was a cause that other doctors and researchers had not considered. Daniels the lead author in the JAMA study would not include this proof of a woman’s pain being generated by intrauterine pressure, so I refused to be author and declined authorship in JAMA. For researchers and physicians that is a ‘big deal’.
In summary, I have not performed a L.U.N.A.procedure in almost 20 years as my research has identified that these women probably have microscopic endometriosis; they do have disregulation of their hypothalamic-pituitary-gonadal (ovarian) axis and abnormalities of their Free Androgen Index which I link to environmental xeno-estrogens (plastics, pesticides, hormones in our food, etc.) Even the worst case of endometriosis in a woman on a morphine drip at Johns Hopkins responded to this combination of FDA meds from 50 years ago. The American College of OB GYN had me present this simple treatment to the other doctors in 2014 at the annual meetin. I am off to lecture European and International doctors in Madrid on August 9-10, 2018. Any readers who would like to see Sheri’s interview about how desperate these women are for pain relief, how they are ignored for 10 years and then left without their female organs and still desperate for someone to believe them, may understand why I have spent 45 years researching and treating my patients. The website is: https://www.TheEndoCure.com. It is part of a larger website that contains links to 5 other research projects/ interests for which there is no pharmaceutical backing. Is DIABETES, CROHN’S DISEASE, HEART DISEASE real but, PMS, Migraine and Endometriosis because they concentrate around women… not as important?
Helen Keller said “Optimism is the faith that leads to achievement. Nothing can be done without hope and confidence” …by the team of the physician and his/her patient.
So, Jim, I hope that next time you do not feed into the same old song and dance that ‘ all doctors are out to make money’ at the expense of ‘women who have nothing else to do but complain’. You are better than that.
Edward Lichten, M.D.
Edward, forgive me for not acknowledging your contribution to the development of LUNA, and thank you for reaching out. I agree that if LUNA had turned out to be effective, it would have been interesting to test whether the effect was mediated via reduced uterine pressure. But Daniels’ JAMA trial was large and pragmatic, so it’s understandable that she didn’t want to include this sort of physiology within it. I’m sorry to hear you fell out over the issue, but It’s good that you have also abandoned the procedure.
Did I read your website https://www.TheEndoCure.com correctly as advocating nandrolone and stanozolol as non-surgical treatments for endometriosis and pelvic pain? I couldn’t find either a Cochrane review nor any randomised trials of their effectiveness for these conditions. Have I missed them? Do you have a link?